
Victor Chukwudi Osamor
Bioinformatics Unit, Department of Computer and Information Sciences, College of Science and Technology, Covenant University, Ota, Ogun State, Nigeria
Biotechnology
Year: 2010 | Volume: 9 | Issue: 2 | Page No.: 196-203







ABSTRACT
In recent years, several significant objectives and initiatives relevant to the global malaria problem have affirmed the challenge of malaria. The specific objectives, initiatives and resolutions form the basis for the development of and the setting of priorities under the Malaria Plan in most countries. Since malaria management entails the care and good handling of both asymptomatic and symptomatic malaria infection, the development and use of drugs and vaccines becomes very important. This study identified and assessed the roles of global initiatives and local efforts in evolving malaria treatment discovery especially through drug and vaccine development and delivery in Africa. In this study, we concluded that the global initiatives are great stimulant that catalyze local efforts in most African countries and hence determines the extent of success or failure each local malaria management efforts. This may be partly because the strategic planning and funding are provided to these low-income countries with high malaria burden. The author, while identifying some level of weakened coordinated R and D in Africa sought for an intensified involvement of global initiatives in sterile insect technique in integrated malaria vector control.
PDF Abstract XML References Citation
How to cite this article
Victor Chukwudi Osamor, 2010. Global Initiatives and Local Efforts Towards Management of Malaria in Africa. Biotechnology, 9: 196-203.
DOI: 10.3923/biotech.2010.196.203
URL: https://scialert.net/abstract/?doi=biotech.2010.196.203
DOI: 10.3923/biotech.2010.196.203
URL: https://scialert.net/abstract/?doi=biotech.2010.196.203
INTRODUCTION
Several global initiatives are committed to malaria treatment discovery through several policy statement, objectives and/or activities through public-private partnership. The antimalarial drug/ vaccine development can follow several strategies, ranging from minor modifications of existing agents to the design of novel agents that act against new targets, as available agents are being combined to improve antimalarial regimens (Rosenthal, 2003). Among important efforts that are currently ongoing are the optimization of therapy with available drugs, including the use of combination therapy, the development of analogs of existing agents, the discovery of natural products, the use of compounds that were originally developed against other diseases, the evaluation of drug resistance reversers and the consideration of new chemotherapeutic targets. The last category benefits from recent advances in malaria research technologies and genomics and is providing new classes of drugs (Rosenthal, 2003).
Discovery of new malaria treatment benefits from recent advances in malaria research technologies and genomics and is providing new classes of drugs. A number of new antimalarial therapies will likely be needed over the coming years. So, it is important to pursue multiple strategies for drug discovery. The development of resistance in the parasite to effective and inexpensive drugs, the lack of a licensed malaria vaccine and the fundamental complexity inherent in the malaria parasite means that there is an urgent need to better understand the function of P. falciparum genes and their biological role to support the development of new and effective antimalarial strategies (Le Roch et al., 2003). For example, Fig. 1 shows a current typical WHO/TDR drug discovery pipeline from genomics to preclinical development stage (Nwaka, 2008).
It is imperative to investigate the relevance of these global initiatives and their role in effective malaria management especially in a developing country like Nigeria. This will help to evolve strategies and implementation of objectives beneficial to formidable malaria control.
BASIC GLOBAL INITIATIVES
In order to be able to carry out effective study of the dynamics of malaria management to analyse the level of local efforts in malaria control, we identified the various global initiatives set up to tackle the problem of malaria. Emphasis was paid more to the initiatives that has been quite notable for very regular malarial activities, this is nevertheless non-exhaustive and there are cases where their objectives expanded beyond malaria solution provisions. Below are the basic global initiatives responsible for value- added services in form of funding, material provision (bednet), R and D, education and training to malaria endemic regions of Africa and the world. The method adopted is the creation of research partnerships within and outside of Africa and technology transfer through inter- and multi-country research projects and network.
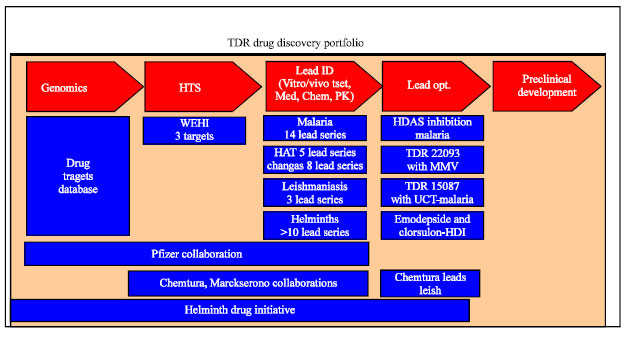 | |
| Fig. 1: | TDR drug development pipeline and portfolio with genomics at the basics (Source: Nwaka, 2008) |
The united nations millennium development goals (MDG) (September, 2000): The malaria plan of MDG is to halt and begin to reverse the incidence of malaria (and other major diseases) by 2015. The malaria fight by MDG is reflected in Goal 6 of their 8 goals mandate as listed in that subsequent paragraph below. MDG refers to eight goals that respond to the world's main developmental challenges to be achieved by 2015. The eight MDGs break down into 21 quantifiable targets that are measured by 60 indicators. These goals were drawn from Millennium Declaration that was adopted by 189 nations-and signed by 147 heads of state and governments during the UN Millennium Summit in September 2000. Listed in definite order, these eight goals (http://www.undp.org/mdg/basics.shtml,2009) are:
| Goal 1: | Eradicate extreme poverty and hunger |
| Goal 2: | Achieve universal primary education |
| Goal 3: | Promote gender equality and empower women |
| Goal 4: | Reduce child mortality |
| Goal 5: | Improve maternal health |
| Goal 6: | Combat HIV/AIDS, malaria and other diseases |
| Goal 7: | Ensure environmental sustainability |
| Goal 8: | Develop a global partnership for development |
The Roll Back Malaria (RBM) initiative: The RBM was established in October, 1998 by WHO, UNICEF, UNDP and the World Bank, in an effort to provide a coordinated global response to Malaria disease. However, RBM target is to halve the malaria burden in participating countries through interventions that are adapted to local needs and reinforcement of the health sector by 2010. Today, RBM Partnership forges a world-wide consensus among over 1000 partners and mobilise resources to achieve jointly malaria control targets in support of progress towards MDGs and Malaria Eradication Agenda (malERA). RBM's overall strategy aims to reduce malaria morbidity and mortality by reaching universal coverage and strengthening health systems. The RBM's Global Malaria Action Plan (GMAP) defines three stages of malaria control: (1) scaling-up for impact (SUFI) of preventive and therapeutic interventions, (2) sustaining control achievements over time; (3) initiate regional elimination efforts. Currently, RBM is working vigorously to reach its mandate through a new innovation of creating for the nomination of Research and Academia Constituency to add to its processes.
The Global Malaria Control Strategy (GMCS): GMCS was established in October (1992) to:
| • | Provide early diagnosis and prompt treatment |
| • | Plan and implement selective and sustainable preventive measures, including vector control |
| • | Detect early, contain or prevent epidemics |
| • | Strengthen local capacities in basic and applied research to permit and promote the regular assessment of a country’s malaria situation, in particular the ecological, social and economic determinants of the disease |
Malaria research reference reagent resource center (MR4): MR4 is a biological resource center providing research reagents for free to malaria scientists. MR4 serves the malaria research community by providing reagents and training. It has a collection of well characterized research materials that are responsive to specific requests and research projects. The MR4 is located at the American Type Culture Collection (ATCC) in Manassas, Virginia, US.
Multilateral Initiative on Malaria (MIM): Multilateral Initiative on Malaria (MIM) was established in 1997 with a mission to strengthen and sustain the capacity of malaria-endemic countries in Africa to carry out research required to develop and improve tools for malaria control. This is done through collaborative research and training. MIM/TDR is embedded in UNICEF/UNDP/World Bank/WHO Special Programme for Research and Training in Tropical Diseases. MIM/TDR evaluates research grant applications from African malaria scientists and awards funds via a competitive peer-review process. MIM contributes to global efforts to address the problem of malaria by facilitating the emergence of dynamic malaria research networks and collaboration with malaria control programs in Africa through the following objectives:
| • | Developing sustainable malaria research capacity in Africa-through international and Pan-African scientific partnerships and training |
| • | Promoting global communication and cooperation-between institutions to avoid duplication of effort |
| • | Ensuring research findings are applied to malaria treatment and control |
| • | Raising international public awareness of the problem of malaria-to raise the status of malaria on political agendas to mobilize resources and action (http://www.mimalaria.org/eng/aboutmim.asp) |
Medicine for Malaria Venture (MMV): The MMV was established in October, 1999. It is a Swiss non-profit initiative that operates as a public-private partnership for R and D and production of efficacious malaria drugs.
DRUGS AND VACCINES FOR MALARIA TREATMENT
Some available drugs: Drugs are chemicals or other substances that alter the function of an organism and are referred as medicines or therapeutic drugs when used for the prevention, treatment and alleviation of diseases as opposed to other hard drugs, such as opiates, which are used illegally. Drugs can be derived from plant, mineral,animal, or synthetic sources.
| Table 1: | Some available malaria drugs showing evolution with time |
 | |
Many early folk medicines, including aspirin, opium and quinine were derived from plants. Minerals used as medicines include boric acid, Epsom salts and iodine. Many hormones used to treat a bodily malfunction include insulin for diabetes, or growth hormone to promote proper human development. Table 1 shows the list of some available malaria drugs as they evolve with time and fail due to resistance, non-compliance, safety and formulation issues (Nwaka, 2008). The table also shows respective organizations involved in various antimalarial drug development.
Natural products are the sources of the two most important drugs currently available to treat severe P. falciparum malaria, quinine and derivatives of artemisinin. In the case of artemisinin, relatively simple chemical modifications of the natural product parent compound have led to a series of highly potent antimalarials that are playing an increasingly important role in the treatment of malaria (Meshnick, 2001). However, the cost of these compounds may be limiting and so efforts to design fully synthetic endoperoxides that are less expensive to produce are an important priority (Posner et al., 2003; Vennerstrom et al., 2000).
Artesunate has been studied in combination with both sulfadoxine/pyrimethamine (Von Seidlein et al., 2000) and amodiaquine (Adjuik et al., 2002) in Africa, with good efficacy. Rosenthal (2003) stated that artemisinin analogs, in particular artesunate and artemether, have recently shown great promise as rapidly acting as potent antimalarials, but the short half-lives of these compounds lead to many late recrudescences after therapy, as seen with artesunate/sulfadoxine/pyrimethamine in Uganda (Dorsey et al., 2002) suggesting that combination therapies are necessary to fully exploit the potency of this class.
Ideally, a combination regimen that prevents resistance development should include at least two agents against which parasite resistance has not yet developed and which have similar pharmacokinetics, so that low blood levels of a single agent will not be present. No such ideal regimen is currently available, although chlorproguanil/dapsone/artesunate may prove to fit this description. Alternatively, the combination of a short-acting, highly potent compound and a longer-acting agent may prove effective, if the initial decrease in parasite burden is so great as to limit subsequent resistance development to the long-acting agent (e.g., artesunate/mefloquine). As another alternative, two drugs with similar pharmacokinetics may prove effective even if resistance to each agent is present in the community (e.g., amodiaquine/sulfadoxine/pyrimethamine). Relatively slow-acting antimalarials (e.g., antibiotics) in combinations like quinine and doxycycline may be effective (Rosenthal, 2003).
Initiatives like Medicine for Malaria Venture (MMV) had projects with drugs at various stages of development as at second quarter of 2008 (Fig. 2) (Bathurst, 2008). In Fig. 2, we have the cherry taste and powdery form of Coartem dispersible (from Norvatis), newly formulated for children now at regulatory stage and waiting to be recognized for usage soon. Also Azithromycin CQ is formulated to be safer antimalarial at pregnancy. They all pass from exploratory to regulatory stages of drug development pipeline.
Malaria drug resistance issues: Complicating the process of developing new drugs and treatment strategies for malaria is the problem of drug resistance issues. This is made worse particularly in the issue of resistance to the most affordable drugs such as chloroquine and Fansidar® (a combination drug of pyrimethamine and sulfadoxine are now widely spread). Some progress has been made in studying the mechanisms of drug action and drug resistance in malaria parasites, particularly in Plasmodium falciparum. These efforts are highlighted by the demonstration of mutations in the parasite’s dihydrofolate reductase (DHFR) and dihydropteroate synthase (DHPS) genes conferring resistance on pyrimethamine and sulfadoxine respectively and by the discovery of mutations in the gene coding for a putative transporter, PfCRT, conferring resistance on chloroquine. Mutations in a homologue of a human multiple-drug-resistant gene, PfMDR1, have also been shown to be associated with responses to multiple drugs (Hayton and Su, 2004). However, except in the case of resistance to antifolate drugs, the mechanisms of action and resistance to most drugs currently in use are essentially unknown or are being debated. But it is believed that there are many more novel ways the parasite uses to engender resistance to drugs.
Vaccines: Zakeri et al. (2007) stated that most experimental pre-erythrocytic stage vaccines are based or include the circumsporozoite protein (CSP) as an immunogen (any substance or organism that provokes an immune response (produces immunity) when introduced into the body). CSP is the dominant surface protein of the sporozoite and it is used for formulations targeting the pre-erythrocytic stages (the sporozoite and the liver stage parasite).
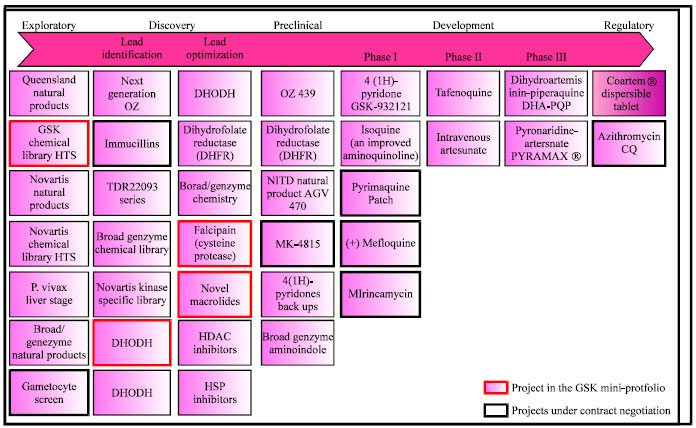 | |
| Fig. 2: | Medicine for Malaria Venture (MMV) initiative drug discovery portfolio (Source: Bathurst, 2008) |
The gene coding for CSP was the first Plasmodium gene to be isolated and characterized (Dame et al., 1984; Ellis et al., 1983) and the first P. falciparum subunit vaccine tested in human volunteers was based on this protein (Herrington et al, 1987). Today, the most advanced vaccine against malaria, RTS, S, is based on the P. falciparum CSP (PfCSP) (Gordon et al., 1995). This vaccine has already undergone two Phase IIb clinical trials in adults and children from The Gambia and Mozambique, respectively (Alonso et al., 2004; Bojang et al., 2001) where it provided modest levels of protection. Other examples include, multistage DNA vaccine combination (MuStDO), apical membrane antigen 1 (AMA 1), TRAP/SSP2, synthetic peptide vaccine (SPf66), etc. Generally, protein-based vaccines, DNA-based vaccines, naturally acquired immunity (NAI) and immunisation with irradiated sporozoite confers partial immunity in rodent and humans (Richie and Saul, 2002).
LOCAL EFFORTS AND APPROACHES
Despite the challenges of malaria, some level of results has been achieved towards its eradication. It has been observed that the several global initiatives on malaria have been a great catalyst on the activities of the local people towards effective malaria management in their area. The impact of these, has also given rise to several networks which are collection of people with same goal to eradicate malaria across Africa.
Management strategies and control efforts in Nigeria
Coordinated biotechnology research and development: Across Africa with particular focus on Nigeria, coordinated research seem to be weakened partly because of great disparity in the level of knowledge of biotechnology among various research clusters and lack of research infrastructures. In our work (Daramola et al., 2008), we designed and assessed the implementation of a National Health Care grid infrastructure for a developing nation like Nigeria taking cue with what obtain in other advanced countries. This will definitely combine the use of wireless technology, Internet, sensor network and software development technique for large applications similarly applicable to the work in Osamor et al. (2010b). This will help to alleviate the treatment of malaria in urban and remote areas of the country where medical services would have been scare and ultimately health care grid infrastructure will help in national planning. The complexity of malaria and the need to monitor the transmission progression has also stimulated research in microarray technology (Osamor, 2009a, b). The analysis of the microarray data of malaria origin requires extensive bioinformatics techniques and we apply k-means clustering to study the underlying malaria transmission mechanism (Osamor et al., 2010a, b). In other to handle large data analysis at effective and efficient time, we developed an algorithm called MMkmeans (Osamor et al., 2009a, b, 2010a) for clustering malaria microarray data and also validated it for purposes of revealing underlying information about the disease (Osamor et al., 2009b, 2010a). The good knowledge of the mechanism of transmission will be useful in the design of effective therapeutics and diagnostics for cure and eradication as demonstrated in Osamor (2009b).
While considering the ethical and social aspects of irradiation of male Anopheles mosquitoes in integrated control of malaria vectors, Osamor (2010) noted that the technique introduces genetic sterility in anopheline females of the target population in the field following their mating with released sterile males. Sterility is caused by dominant lethal mutations in the sperm of the released males resulting from radiation leading to the death of the developing zygote in female Anopheles mosquitoes. Based on the geographical and etiological setting of Nigeria, we discovered that the involvement and provision of support for sterile insect technology (SIT) by global initiatives in Nigeria will advance the search for cure of malaria (Osamor, 2010). The ongoing and next level of study is the development and delivery of a PCR-based biochip automation for diagnostics purposes of malaria patients.
Scattered research efforts: In Nigeria, malaria control activities are planned and implemented through the Primary Health Care (PHC) system (FMOH, 2005). However, the use of health centers, as the first resort for malaria management has been shown to be low in many African studies including Nigeria. Mothers' malaria treatment-seeking behaviour in rural south-western Nigeria revealed that more than 80% of malaria episodes received treatment outside of the existing government healthcare system (Olaogun et al., 2005; Ajayi and Falade, 2006). The option of malaria treatment at PHC is delayed till the advent of complication and near death. This was attributed to difficulty with access to health centre, scarcity of affordable drugs including antimalarial drugs, perceived deficiencies in the performance of formal health services including poor clinical skills, attitude of health personnel and cultural beliefs (WHO/UNICEF, 2003; Feyisetan et al., 1997). This practice increases morbidity and mortality in addition to contributing to possible emergence of drug resistance (WHO/UNICEF, 2003; Ajayi et al., 2008).
World Health Organisation (WHO) initiated the Roll Back Malaria (RBM) Programme in 1998 to halve malaria death world-wide by 2010 (Nabarro and Tayler, 1998) with interventions such as home management of malaria (HMM) (early and appropriate treatment of malaria especially for children less than five years old); Intermittent Preventive Treatment (IPT) of malaria for pregnant women; insecticide treated nets and artemisinin-based combination therapy (ACT) replacing chloroquine and sulfadoxine-pyrimethamine that exhibit parasite resistance (Attaran et al., 2004).
With the approach of 2010 deadline for Roll Back Malaria (RBM), a pilot study was conducted by Adeneye et al. (2007) to assess the awareness, accessibility and use of malaria control strategies among at-risk groups within the context of RBM in Nigeria holo-endemic community, Ijebu-Igbo, in Ogun State, Nigeria. Their results showed that 14.7 and 16.2% of all classes of respondents interviewed were aware of the Home Management of Malaria (HMM) and new antimalarial drug policy programme. Also 63.5% knew about insecticide treated nets (ITNs), while only 22.1% was using the treated material. Only 5.8% of mothers of children less than five years old and none of the pregnant women had taken the new combination drug (ACT). Eight (23.5%) of the 34 pregnant women interviewed knew about intermittent preventive treatment of malaria for pregnant women (IPT). The results of this pilot study showed that efforts need be intensified to make adequate information and materials relating to the different malaria control strategies more available and accessible at the community level to achieve and sustain the RBM goals, both in Ogun State and in Nigeria in general (Adeneye et al., 2007) (Fig. 3).
The Nigerian Government after 2000 Abuja Declaration, where African Governments agreed to support the RBM strategy of at least 60% at risk-population sleep under ITN, has been promoting RBM interventions through the NetMark initiative (a United States Agency for International Development-funded public-private partnership. Nigeria’s national policy on malaria treatment in 2004 dropped chloroquine and adopted the combination therapy of artemether and lumefantrine (Coartem), artesunate and amodiaquine (Adeneye et al., 2007).
Ajayi et al. (2008) confirmed earlier reports that majority of treatment for malaria take place in the home with drugs bought from drug vendors and proposed the evaluation of intervention (health education plus treatment guideline developed using participatory approach) in the use of artemisinin based combination drugs such as artemether-lumefantrine which is now the drug of choice in the treatment of acute uncomplicated malaria in Nigeria.
African networks: A part WHO/TDR initiative, African Network for Drugs and Diagnostics Innovation (ANDI) was launched in Abuja in 2008 (http://www.meeting.tropika.net/andi/,2009) to promote and sustain African-led R and D innovation through the discovery, development and delivery of affordable new tools including those based on traditional medicines.
 | |
| Fig. 3: | Malaria Control Strategies Awareness Level in parts of Ogun State, Nigeria (Adapted from Adeneye et al., 2007) |
Malaria treatment discovery is one of the major challenges before this initiative. Osamor 2009a), emphasized the seriousness of institutions and governments in Africa towards eradicating malaria through the use of genomics techniques and microarray technology by citing the interest of The New Partnership for Africa’s Development (NEPAD) and WHO/TDR efforts in capacity building in the continent. Examples include the setting-up of ACGT Microarray and African Biosciences facilities in South Africa; series of conferences and workshops organized by African Society of Bioinformatics and Computational Biology (ASBCB).
African Malaria Network Trust (AMANET): In 1995, African Malaria Vaccine Testing Network (AMVTN) started its activities but later metamorphosed into The African Malaria Network Trust (AMANET) in 2002. Their initial primary goal is preparation of Africa in planning and conducting malaria vaccine trials but have now expanded beyond that singular goal in malaria interventions to incorporate an integrated approach. These include creation of global awareness of the African malaria burden, advancement of essential human capacity for research and development of malaria intervention in Africa, determination of the needs and characterisation of potential sites for testing malaria interventions in Africa and promotion of good governance, efficient management and networking of malaria institutions in Africa (http://www.mimalaria.org/eng/aboutmim.asp). AMANET currently serves as secretariat for MIM since 2006.
Elimination eight (E8) regional initiative: Eight (E8) regional initiative was recently launched in March 3, 2009 by Ministers of health from the eight southern African countries in Windhoek, Namibia. The goal of the meeting was to increase collaboration among the eight neighboring countries, to achieve their common goal of eventual elimination of malaria in the region and elimination in four countries, Botswana, Namibia, South Africa and Swaziland, by 2015. The E8 includes these four countries, along with their other four northern neighbors, Angola, Mozambique, Zambia and Zimbabwe. The idea behind the enlarged Elimination Eight (E8) is that four southernmost malarious countries in southern Africa can only successfully eliminate malaria, if the countries immediately to their north also focus their efforts on scaled-up malaria control along their southern borders. Ministers agreed to strengthen cross-border collaboration, jointly mobilize financial and technical resources to eliminate malaria, build health systems capacity in the region and coordinate multi-sectoral efforts among all partners working on malaria activities. A Ministerial Resolution was subsequently approved by the Southern African Development Community (SADC), in Maputo, Mozambique in April 2009 owing to the formidable interest in malaria elimination in this region.
CONCLUSIONS
While organization on global malaria initiatives discussed may not be exhaustive, the basic initiatives were highlighted. In our study, we conclude that global malaria initiative through several public-private partnership have advanced the development of drugs and current efforts will soon yield an effective vaccine for malaria. It is also true that majority of the activities of the global initiatives occur in low income countries with high endemic level of the disease thereby minimizing the high level devastations occasioned by various intervention measures. Issues of resistance were noted to be a problem in the search for long lasting cure for malaria but Artimisinin-based Combination Therapy (ACT) provides current panacea. However, several Africa Networks are springing up with much hope that more emphasis can be sustained on malaria eradication and guarantee its elimination from the continent. However, its often said that if malaria were to be a white man’s disease, it would have been eradicated long time ago. The rate of coordinated research and synergy amongst Africans in biotechnology, research and development will soon provide answer for the eradication of malaria.
REFERENCES
- Adeneye, A.K., A.S. Jegede, M.A. Mafe and E.E. Nwokocha, 2007. A pilot study to evaluate malaria control strategies in Ogun State, Nigeria. World Health Popul., 9: 83-94.
PubMedDirect Link - Adjuik, M., P. Agnamey, A. Babiker, S. Borrmann and P. Brasseur et al., 2002. Amodiaquine-artesunate versus amodiaquine for uncomplicated Plasmodium falciparum malaria in African children: A randomised, multicentre trial. Lancet, 359: 1365-1372.
Direct Link - Ajayi, I.O. and C.O. Falade, 2006. Pre-hospital treatment of febrile illness in children attending the general outpatients’ clinic. University College Hospital, Ibadan, Nigeria. Afr. J. Med. Med. Sci., 35: 85-91.
Direct Link - Ajayi, I.O., C.O. Falade, E.A. Bamgboye, A.M.J. Oduola and O.O. Kale, 2008. Assessment of a treatment guideline to improve home management of malaria in children in the Rural South-West Nigeria. Malaria J., 7: 24-24.
PubMed - Alonso, P.L., J. Sacarlal, J.J. Aponte, A. Leach and E. Macete et al., 2004. Efficacy of the RTS, S/AS02A vaccine against Plasmodium falciparum infection and disease in young African children: Randomized controlled trial. Lancet, 364: 1411-1420.
PubMedDirect Link - Attaran, A., K.I. Barnes, C. Curtis, U. D'Alessandro and C.I. Fanello et al., 2004. WHO, the global fund and medical malpractice in malaria treatment. Lancet, 363: 237-240.
CrossRef - Bojang, K.A., P.J.M. Milligan, M. Pinder, L. Vigneron and A. Alloueche et al., 2001. Efficacy of RTS, S/AS02 malaria vaccine against Plasmodium falciparum infection in semi-immune adult men in The Gambia: A randomised trial. Lancet, 358: 1927-1934.
Direct Link - Dame, J.B., J.L. Williams, T.F. McCutchan, J.L. Weber and R.A. Wirtz et al., 1984. Structure of the gene encoding the immunodominant surface antigen on the sporozoite of the human malaria parasite Plasmodium falciparum. Science, 225: 593-599.
CrossRefDirect Link - Ellis, J., L.S. Ozaki, R.W. Gwadz, A.H. Cochrane, V. Nussenzweig, R.S. Nussenzweig and G.N. Godson, 1983. Cloning and expression in E. coli of the malarial sporozoite surface antigen gene from Plasmodium knowlesi. Nature, 302: 536-538.
CrossRefDirect Link - Feyisetan, B.J., S. Asa and J.A. Ebigbola, 1997. Mother's management of childhood diseases in Yoruba Land: The influence of cultural beliefs. Health Transit. Rev., 7: 221-234.
PubMedDirect Link - Gordon, D.M., T.W. McGovern, U. Krzych, J.C. Cohen and I. Schneider et al., 1995. Safety, immunogenicity and efficacy of a recombinantly produced Plasmodium falciparum circumsporozoite protein-hepatitis B surface antigen subunit vaccine. J. Infect. Dis., 171: 1576-1585.
Direct Link - Hayton, K. and X.Z. Su, 2004. Genetic and biochemical aspects of drug resistance in malaria parasites. Curr. Drug Targets Infect. Disord., 4: 1-10.
PubMedDirect Link - Herrington, D.A., D.F. Clyde, G. Losonsky, M. Cortesia and J.R. Murphy et al., 1987. Safety and immunogenicity in man of a synthetic peptide malaria vaccine against Plasmodium falciparum sporozoites. Nature, 328: 257-259.
Direct Link - Le Roch, K.G., Y. Zhou, P.L. Blair, M. Grainger and J.K. Moch et al., 2003. Discovery of gene function by expression profiling of the malaria parasite life cycle. Science, 301: 1503-1508.
CrossRefDirect Link - Nabarro, D.N. and E.M. Tayler, 1998. The roll back malaria campaign. Science, 280: 2067-2068.
PubMedDirect Link - Olaogun, A.A.E., O. Ayandiran, O.A. Olasode, A. Adebayo and F. Omokhodion, 2005. Home management of childhood febrile illness in a rural community in Nigeria. Aust. J. Rural Health, 13: 97-101.
Direct Link - Osamor, V.C., 2009. Experimental and computational applications of microarray technology for malaria eradication in Africa. Sci. Res. Essays, 4: 652-664.
Direct Link - Osamor, V., E. Adebiyi and S. Doumbia, 2009. Comparative functional classification of Plasmodium falciparum genes using k-means clustering. Proceedings of the International Association of Computer Science and Information Technology Conference, April 17-20, IEEE Computer Society Press, pp: 491-495.
Direct Link - Osamor, V.C., F.E. Adebiyi and S. Doumbia, 2010. Clustering Plasmodium falciparum genes to their functional roles using k-means. Int. J. Eng. Technol., 2: 215-225.
Direct Link - Osamor, V.C., O.S. Aloba and I.P. Osamor, 2010. From wooden to digital notice board (dnb): Design and implementation for university administration. Int. J. Electr. Comput. Sci., 10: 79-83.
Direct Link - Posner, G.H., I.H. Paik, S. Sur, A.J. McRiner, K. Borstnik, S. Xie and T.A. Shapiro, 2003. Orally active, antimalarial, anticancer, artemisinin-derived trioxane dimers with high stability and efficacy. J. Med. Chem., 46: 1060-1065.
CrossRefDirect Link - Richie, T.L. and A. Saul, 2002. Progress and challenges for malaria vaccines. Nature, 415: 694-701.
CrossRefDirect Link - Rosenthal, P.J., 2003. Antimalarial drug discovery: Old and new approaches. J. Exp. Biol., 206: 3735-3744.
CrossRefDirect Link - Vennerstrom, J.L., Y. Dong, S.L. Andersen, A.L. Jr. Ager and H. Fu et al., 2000. Synthesis and antimalarial activity of sixteen dispiro-1, 2, 4, 5-tetraoxanes: Alkyl-substituted 7, 8, 15, 16-tetraoxadispiro [5.2.5.2] hexadecanes. J. Med. Chem., 43: 2753-2758.
PubMedDirect Link - Von Seidlein, L., P. Milligan, M. Pinder, K. Bojang and C. Anyalebechi et al., 2000. Efficacy of artesunate plus pyrimethamine-sulphadoxine for uncomplicated malaria in Gambian children: A double-blind, randomised, controlled trial. Lancet, 355: 352-357.
Direct Link - Zakeri, S., M. Avazalipoor, A.A. Mehrizi, N.D. Djadid and G. Snounou, 2007. Restricted T-cell epitope diversity in the circumsporozoite protein from Plasmodium falciparum populations prevalent in Iran. Am. J. Trop. Med. Hyg., 76: 1046-1051.
Direct Link